On the March 4th, 2026 hearing for Tim Walz and Keith Ellison before congress on the subject of fraud in Minnesota, Rep. Nancy Mace grilled Walz on the increases in spending on autism in Minnesota. She showed that there was a 34200% increase between 2017 and 2024.
I have to say, Walz disappointed me a bit. He didn’t have a reason for this increase, instead referring to how Minnesota has some of the healthiest kids in the U.S. That may be true, but it still doesn’t explain away the increase.
My goal today is to see if Minnesota is the only one seeing that increase. Minnesota has been the target of the Trump administration’s ire and found itself in the spotlight for fraud. Are other states displaying the same problem and being ignored? Walz seems to think Trump dislikes him personally, and I agree with that..on the surface. Does the data agree?
Minnesota vs. Other States Medicaid / Autism Spending
Finding data for this was, not surprisingly, difficult. I found an on-going project done by the Office of the Inspector General that has completed Applied Behavior Analysis (ABA) Medicaid payment audits on four states – Maine, Colorado, Indiana and Wisconsin. Using their findings and metrics as a baseline, I compared Minnesota’s numbers. Let’s summarize the reports state-by-state.
Maine
First, let’s list out what the OIG found that qualified as an improper payment:
- Required assessments not completed, or signatures missing from assessments
- Session notes did not meet documentation requirements; missing description or services rendered, goals addressed not listed, data collection not completed
- Non-therapy time included in session notes (lunch, naps, breaks)
- Session notes referred to recreational or academic activities that may not qualify
- ITPs missing parent signatures or missing
- Provider credentials missing from documentation
The total amount of improper payments was listed as $45.6M, with $27.8M of this being the federal share and $17.8M being the state share.
The OIG recommended the following to the Maine Department of HHS:
- refund $28,796,366 (Federal share) to the Federal Government for FFS Medicaid payments for RCS services that did not comply with Federal and State requirements;
- exercise reasonable diligence to review and determine whether any of the estimated ($14,163,521 Federal share) in potentially improper payments for RCS services did not comply Maine’s FFS Medicaid Payments for Rehabilitative and Community Support Services (A-01-24-00006) 15 with Federal and State requirements and refund the Federal share of any improper payment amount to the Federal Government;
- provide additional guidance to providers about how to document RCS services, including the information needed in session notes to support RCS services provided, billable RCS service time, and signature requirements; and periodically conduct a statewide postpayment review of Medicaid payments for RCS services, including reviewing medical records, and provide additional training in the areas in which errors were identified by postpayment reviews.
Maine’s HHS agreed to all of the recommendations, and completed a Corrective Action Plan for each bullet.
Wisconsin
The reasons found for improper payments in Wisconsin include:
- Sessions did not support the CPT code billed
- Sessions did not support the number of units billed
- Sessions did not support the dates of service billed
- Signatures were missing on session notes
- Session notes did not contain the full description of services provided, goals addressed or data collected
- Session notes refer to recreational activities that may not have been allowable
- Session notes included non-therapy time
- Sessions were billed with an incorrect rendering provider
The total number of estimated improper payments in Wisconsin was $18.5M, with $12.2M of this being the federal share and $6.3M being the state share.
The recommendations made to the state of Wisconsin’s HHS were as follows:
- refund $12,287,252 (Federal share) to the Federal Government for FFS Medicaid ABA payments that did not comply with Federal and State requirements;
- exercise reasonable diligence to review and determine whether any of the estimated $62,334,835 (Federal share) in potentially improper ABA payments complied with Federal and State requirements and refund the Federal share of any improper payment amount to the Federal Government;
- develop a procedure to verify the provider who rendered the 97153 -focused treatment service and pay the claim based on the rendering provider’s specialty level; and
- periodically conduct a statewide postpayment review of Medicaid ABA payments, including reviewing session notes, and provide training in areas where errors were identified by postpayment reviews.
Wisconsin also mostly agreed with the recommendations and created a corrective action plan. They did take issue with one, stating, “DHS disagrees with the primary inappropriate payment finding with respect to Wisconsin Medicaid providers’ use of CPT code 97155. DHS agrees with the inappropriate payment findings with respect to session notes not supporting billed units, session notes not supporting dates of services paid, and session notes not including signatures of rendering providers. If improper payments exist, DHS will recover them from providers and work with CMS regarding the return of federal funds upon their request”.
Indiana
The reasons for improper payment in Indiana sound pretty familiar:
- Sessions notes did not meet documentation requirements, missing CPT code
- Services were provided by staff lacking proper credentials
- Required diagnostic assessments or treatment referrals were missing
- Session notes did not fully disclose the extend of services provided or did not include a detailed statement on techniques used or duration of services provided
- Session notes include non-therapy time
- Session notes referred to recreational or academic activities that may not be allowable
- Session notes refer to group activities, but payments were made for an individual
Overall, the estimated overpayment number was $56.5M, with $39.4M being the federal share and $17.1M being the state’s.
The following recommendations were made to Indiana’s HHS:
- refund $39,432,556 (Federal share) to the Federal Government for FFS Medicaid ABA payments that did not comply with Federal and State requirements;
- provide additional guidance to ABA facilities for documenting ABA, including services that must be provided to support the use of CPT codes 97155 and 97156, State signature requirements, the detail in session notes needed to support ABA provided, and what the State agency considers billable ABA time;
- periodically perform a statewide postpayment review of Medicaid ABA payments, including reviewing medical records, to educate providers on requirements and to recover payments that did not comply with Federal and State requirements;
- periodically review its prior authorization contractor’s procedures for verifying ABA facilities’ compliance with requirements for State diagnostic evaluations and treatment referrals for ABA; and
- exercise reasonable diligence to review and determine whether any of the estimated $53,236,026 (Federal share) in potentially improper ABA payments complied with Federal and State requirements and refund the Federal share of any improper payment amount to the Federal Government.
Indiana agreed to all recommendations and replied with a corrective action plan. They stated they will first review the claims and, where they find improper payments, they will refund the feds.
Colorado
This all sounds like déjà vu at this point, but nevertheless here are the improper payment categories:
- Sessions notes did not meet documentation requirements, missing CPT codes
- Services were provided by staff without proper credentials
- Required assessments or treatment referrels were missing
- Session notes did not fully describe services provided
- Session notes referred to recreational or academic activities that may not have been allowable
- Session notes included non-therapy time
- Session notes referred to group activities, but payments were made for an individual
In Colorado, the estimated impropler payment figure was $77.8M, with $42.6M being the federal share and $35.2M being the state’s.
The following recommendations were made:
refund $42,649,438 (Federal share) to the Federal Government for FFS Medicaid ABA
payments that did not comply with Federal and State requirements;
- provide additional guidance to ABA facilities on: (1) documenting ABA, including services that must be provided to support the use of CPT code 97155, signature requirements, and the information needed in session notes to support ABA provided; (2) billing ABA, including what the State agency considers billable ABA time; and (3) credentialing requirements for ABA providers;
- periodically perform a statewide postpayment review of Medicaid ABA payments, including reviewing medical records, to educate providers on Federal and State requirements related to documentation and provider credentialing and to recover payments that did not comply with Federal and State requirements;
- periodically review its prior authorization contractor’s procedures for verifying ABA facilities’ compliance with requirements for State diagnostic evaluations and treatment referrals for ABA; and
- exercise reasonable diligence to review and determine whether any of the estimated $112,542,978 (Federal share) in potentially improper ABA payments complied with Federal and State requirements and refund the Federal share of any improper payment amount to the Federal Government.
Colorado was a little more feisty than the other states when it came to addressing the recommendations. On the first recommendation, Colorado flatly disagreed and stated OIG did not provide enough line-by-line information to substantiate a repayment, and stated they will validate these claims before committing to repayment. Recommendations 2-4 were agreed with, and recommendation 5 was partially agreed with on the same basis for disagreeing with recommendation 1 – not enough information, more validation needed.
ABA Billing Requirements
Now that we have an understanding of what issues exist in states where a full audit was conducted, I’m wondering – what are the requirements for an ABA claim to be reimbursable? Using the BCBS guidelines, the requirements are:
- Provider must be a qualified healthcare professional (QHP) certified by the Behavior Analyst Certification Board (BACH) as a Behavior Analyst, a Licensed Behavior Analyst, or a Licensed Psychologist.
- ABA must not be provided for educational, vocational, respite, or custodial purposes
- Services must take place in a home, office, or school setting
- Every rendered service must be supported by: a parent/caregiver signature including the service code, provider name/credentials, place of service, date, and start/end times; a written session note; and data points available for audit purposes. Session notes must reflect that both the provider and patient were present for the entire encounter.
- Only direct, face-to-face treatment may be reimbursed
- CPT codes 97151, 97153, 97154, 97155, 97156, 97158, 032T, and 0373T are eligible
- For parent education, only 1 hour per week may be billed
- Billing must take place in 15 minute increiments
- Direct supervision is separately billed, indirect supervision is considered a bundled practice and is not billable.
In addition, each state is responsible to perform an annual post-payment audit.
So, not we know what the requirements are for claiming reimbursement for ABA. This shows that the issues with the four states we looked at is not an issue of improper guidance from the federal level, it is indeed a state-level implementation problem.
Minnesota Medicaid Spending vs. Everyone Else
Unfortunately, since Minnesota has not been audited by the OIG, the level of detailed information I could find for the previous four states is not available. Instead, I will look at overall ABA/ Fee-For-Service spending increase % for each state.
WARNING: Some really, really deep data nerdery is about to take place. Please ensure you are wearing the proper PPE of thick rimmed glasses, pocket protectors and your inhaler. 😉
This data required that I download the entirety of the Medicaid Spending Data from HuggingFace, provided directly from the HHS. HuggingFace is a data repository commonly used and populated by amatuer and professional researchers. I worked on a research team out of Princeton, NJ and had my share of HuggingFace encounters in my research. Data is only available from 2018-2024, and was quite limited for 2024 so I opted to use 2019 for a better picture.
I used MySQL to create a table of total spending by provider ID where the CPT codes matched the ABA CPTs as listed above, then used Excel-foo to VLOOKUP where each provider is located. This allowed me to calculate the total number of providers in each state, then look at the percent change from 2019 to 2024.
It’s pretty significant.
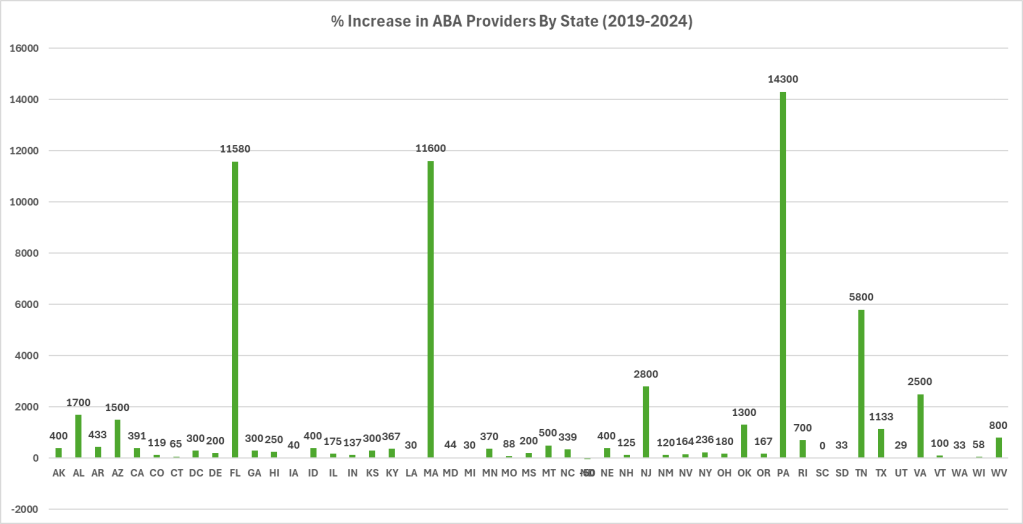
Those are PERCENTAGES. You’ll notice that Minnesota did not NEARLY experience the increase in percentage of providers billing against ABA codes as in other states.
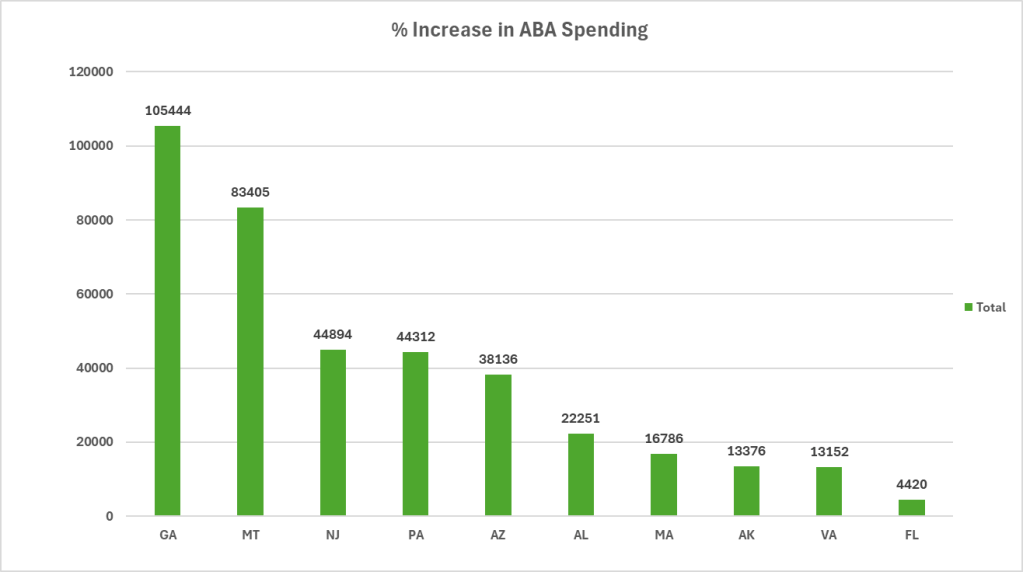
Next, I calculated the total increase in paid out claims from 2019 to 2024 using the same methodology. The increases were so astronomically large, I couldn’t even put it on the same chart.
One thing I did have to the is remove states that received no finding in 2019. This is because the percentage increase is misleading as a single dollar of funding would be a 100% increase. Here is the top 10 chart by increases in ABA spending. Again, these are percentages.
For those interested, here is the data table for all states sorted from most to least increase.
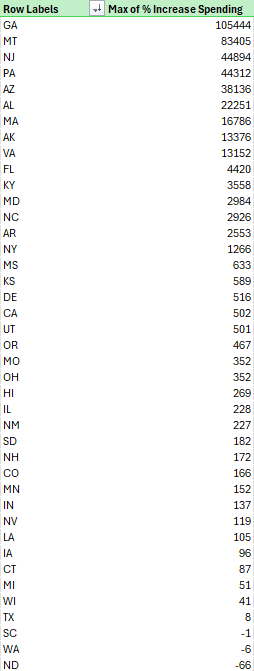
Minnesota is 13th from the last in terms in increase from 2019’s spending the 2024’s. WHAT?!
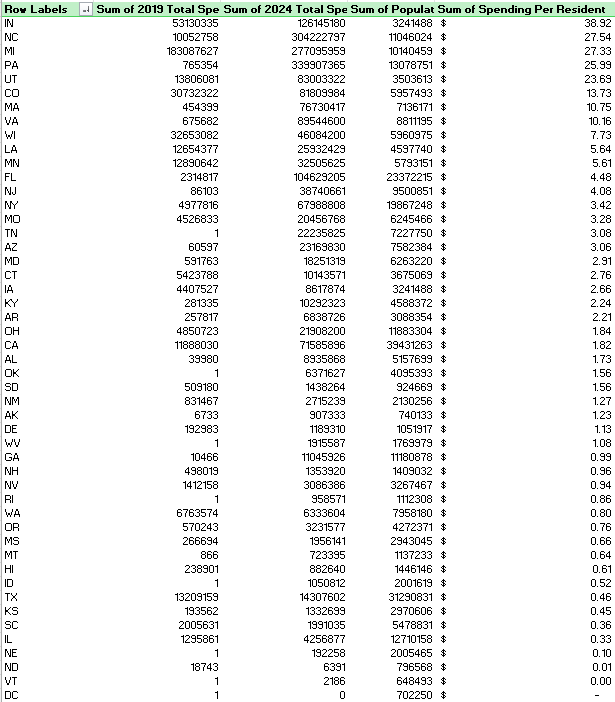
As my awesome reader Derik pointed out in the comments below, percentages can be very deceiving. I created a data table the showed 2019 and 2024 spending, along with population of the state in 2024 and spending per resident for an additional reference. Here it is, straight from the pivot table (states with no spending in 2019 removed, again)
Conclusion
I’m honestly even more confused than I was before I did this research. Minnesota’s increase from 2017-2019 must have been INCREDIBLY high for Mace’s numbers to make ANY sense. Or, she pulled them out of her ass. *shrug*
Walz might be onto something that Trump just hates him personally, because the numbers show we have WAY bigger problems elsewhere.
If you’d like to repeat my experiments, I can send you my data tables!
❤

Leave a comment